

All India Postal Employee Union, Gr-C is the major constituent of National Federation of Postal Employees - The biggest Federation of the Largest Postal Network of the World highlighting the principles of unity and struggle for the advancement of postal workers
Wednesday, 30 June 2021
NFPE Odisha welcomes Shri Sanjiv Ranjan, PMG, Berhampur Region

Shri Sanjiv Ranjan (IPoS:1996) PMG, South Bengal Region, Kolkata joins today (30.06.2021) as Postmaster General, Berhampur Region on transfer vide Directorate Order No. 1-1/2021-SPG, dated 31.05.2021.
NFPE, Odisha extends a warm welcome to the new PMG to Odisha, the holy land of Lord Jagannath and expects that not only Berhampur Region but Odisha Postal Circle will add a lot to its glorious history.
= B SAMAL =
Circle Secretary, AIPEU, Gr-C &
Leader, RJCM (Staff Side), Odisha
Consumer Price Index for Industrial Workers (2016=100) – May, 2021
Ministry of Labour & Employment
Consumer Price Index for Industrial Workers (2016=100) – May, 2021
Posted On: 30 JUN 2021 5:13PM by PIB Delhi
Key Points
- All-India Consumer Price Index for Industrial Workers (2016=100) for May, 2021 increased to 120.6 points compared to 120.1 points for April 2021.
- The increase observed in index is mainly due to Food & Fuel items like Rice, Arhar Dal, Masur Dal, Fish Fresh, Goat Meat, Eggs-Hen, Edible Oil, Apple, Banana, Jamun, Papaya, Potato, Tomato, Brinjal, Cabbage, French Bean, Garlic, Onion, Sugar White, Tea-leaf, Cooking Gas, Kerosene Oil, Petrol, etc. which experienced an increase in prices.
- Inflation for May, 2021 went up to 5.24 per cent compared to 5.14 per cent of previous month. Similarly, Food inflation also increased to 5.26 per cent from 4.78 per cent in the previous month.
The All-India CPI-IW for May, 2021 increased by 0.5 points and stood at 120.6 (one hundred twenty and point six). On 1-month percentage change, it increased by 0.42 per cent with respect to previous month compared to an increase of 0.30 per cent recorded between corresponding months a year ago.
The maximum upward pressure in current index came from Food & Beverages group contributing 0.35 percentage points to the total change. At item level, Rice, Arhar Dal, Masur Dal, Fish Fresh, Goat Meat, Eggs-Hen, Edible Oil, Apple, Banana, Jamun, Papaya, Potato, Tomato, Brinjal, Cabbage, French Bean, Garlic, Onion, Sugar White, Tea-leaf, Cooking Gas, Kerosene Oil, Mobile Telephone Charges, Petrol, etc. are responsible for the rise in index. However, this increase was mostly checked by Leechi, Mango, Water Melon, Bitter Gourd, Lady’s Finger, Lemon, Parwal, Torai, Tamarind, etc. putting downward pressure on the index.
At centre level, Coonoor recorded maximum increase of 4.1 points followed by Udham Singh Nagar with 3.6 points. Among others, 4 centres observed an increase between 2 to 2.9 points, 18 centres between 1 to 1.9 points and 41 centres between 0.1 to 0.9 points. On the contrary, Bhilwara recorded a maximum decrease of 1.2 points followed by Amritsar with 1 point. Among others, 17 centres observed a decline between 0.1 to 0.9 points. Rest of 4 centres remained stationary.
Year-on-year inflation for the month stood at 5.24 per cent compared to 5.14 per cent for the previous month and 5.10 per cent during the corresponding month an year before. Similarly, Food inflation stood at 5.26 per cent against 4.78 per cent of the previous month and 5.88 per cent during the corresponding month an year ago.
Y-o-Y Inflation based on CPI-IW (Food and General)

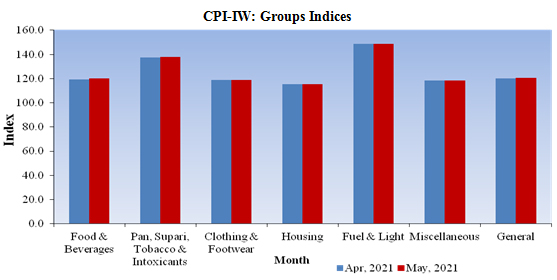
All-India Group-wise CPI-IW for April and May, 2021
Sr. No. | Groups | Apr, 2021 | May, 2021 |
I | Food & Beverages | 119.1 | 120.0 |
II | Pan, Supari, Tobacco & Intoxicants | 137.3 | 137.8 |
III | Clothing & Footwear | 119.0 | 119.0 |
IV | Housing | 115.2 | 115.2 |
V | Fuel & Light | 148.7 | 148.9 |
VI | Miscellaneous | 118.3 | 118.6 |
| General Index | 120.1 | 120.6 |
CPI-IW: Groups Indices
The next issue of CPI-IW for the month of June, 2021 will be released on Friday 30th July, 2021. The same will also be available on the office website www.labourbureaunew.gov.in.
While releasing the index, Minister of Labour & Employment Shri Santosh Gangwar said that the rise in index will result into increased wages of working Class population by way of increase in dearness allowance payable to them.
Shri Gangwar also said that Increase in wages will provide respite to working class families who have witnessed many hardships during the Lockdown period due to COVID. Shri DPS Negi Director General, Labour Bureau said that the rise in Index during May, 2021 is in line with all other price indices compiled and released by different agencies in the country and Marginal increase in annual inflation has, however, been observed during the month due to increase in prices of Food and Fuel items which is also in line with other price indices.
The Labour Bureau, an attached office of the M/o Labour & Employment, has been compiling Consumer Price Index for Industrial Workers every month on the basis of retail prices collected from 317 markets spread over 88 industrially important centres in the country. The index is compiled for 88 centres and All-India and is released on the last working day of succeeding month.
COVID19: Myth vs. Facts
Ministry of Health and Family Welfare
COVID19: Myth vs. Facts
COVID-19 in children is often asymptomatic and seldom requires hospitalization: Dr. V. K. Paul, Member, NITI Aayog
Healthy children recovered with mild illness without need for hospitalization as compared to those who either had comorbidities or low immunity: Dr. Randeep Guleria, Director AIIMS, New Delhi
Covaxin trials have been started on children aged between 2 – 18 years: Dr. N. K. Arora, Chairperson of the COVID-19 Working Group of NTAGI
Detailed guidelines on ‘Management of COVID-19 in children (below 18 years)’ issued by Union Health Ministry
Posted On: 30 JUN 2021 3:32PM by PIB Delhi
Government of India has been at the forefront of the fight against the COVID-19 pandemic. Vaccination forms an integral component of the five-point strategy of Government of India to fight the pandemic (including Test, Track, Treat and COVID Appropriate Behaviour).
During the COVID-19 second wave in the country, several questions have been raised in the media regarding higher vulnerability of children to get adversely impacted by COVID-19 during the subsequent waves, if any.
Experts have allayed these fears and apprehensions on several platforms.
Dr. V. K. Paul, Member (Health), NITI Aayog at the Union Health Ministry's media briefing on COVID-19 on 1st June 2021 had informed that adequate arrangements are being made in terms of healthcare infrastructure in order to provide effective care and treatment to children who may get infected. He had further said that COVID-19 in children is often asymptomatic and seldom requires hospitalization. However, it is possible that a small percentage of children who get infected may need hospitalization
(https://pib.gov.in/PressReleasePage.aspx?PRID=1723469 )

During the media briefing on COVID-19 held on 8th June 2021, Dr. Randeep Guleria, Director, All India Institute of Medical Sciences (AIIMS) New Delhi stated that there is no data, either from India or globally, to show that children will be seriously infected in subsequent waves. Giving further clarification on the issue he said that healthy children recovered with mild illness without need for hospitalization while the ones admitted in the hospital due to COVID19 infection during the second wave in India either had co-morbidities or low immunity (https://www.pib.gov.in/PressReleasePage.aspx?PRID=1725366 )
Dr N K Arora, Chairperson of the COVID-19 Working Group of the National Technical Advisory Group on Immunization (NTAGI) had stated on 25th June 2021 that Covaxin trials have been started on children aged between 2 – 18 years and the results for the same will be received by September to October this year. He said that children may catch the infection, but they will not get seriously ill.
(https://pib.gov.in/PressReleseDetailm.aspx?PRID=1730219 )
Keeping in mind the preparedness that is required to keep the children safe and healthy during subsequent COVID-19 waves, the Union Ministry of Health and Family Welfare has issued guidelines for ‘Management of COVID-19 in children (below 18 years) on 18th June 2021. The document provides detailed guidance on symptoms, various treatments, monitoring and management including Infection Prevention and Control (IPC), advice for using masks etc.
(https://www.mohfw.gov.in/pdf/GuidelinesforManagementofCOVID19inCHILDREN18June2021final.pdf )
The Union Health Ministry and various experts have regularly emphasised the need for COVID Appropriate Behaviour (CAB) for children as well as adults to break the chain of transmission of the virus.
*****
No scientific evidences found linking COVID19 vaccination with infertility in men and women
Ministry of Health and Family Welfare
COVID19 Vaccination: Myths vs. Facts
No scientific evidences found linking COVID19 vaccination with infertility in men and women
COVID-19 vaccination is recommended for all lactating women
Posted On: 30 JUN 2021 3:27PM by PIB Delhi
There have been media reports expressing concerns regarding infertility due to COVID-19 vaccination amongst population of reproductive age and whether COVID-19 vaccination is safe for lactating women.
The Union Ministry of Health and Family Welfare (MoHFW) has clarified in the FAQs posted on the website (https://www.mohfw.gov.in/pdf/FAQsforHCWs&FLWs.pdf) that none of the available vaccines affects fertility of either men or women, as all vaccines and their constituents are tested first on animals and later in humans to assess if they have any such side effects. Vaccines are authorized for use only after their safety and efficacy is assured.
Furthermore, in order to curb the prevalent myth regarding infertility due to COVID-19 vaccination, the Government of India has clarified (https://twitter.com/PIBFactCheck/status/1396805590442119175) that there are no scientific evidences suggesting COVID-19 vaccination can cause infertility in men and women. The vaccines have been found to be safe and effective.

In a recent interview, Dr. N. K Arora, Chairperson of COVID-19 Working Group of National Technical Advisory Group on Immunization (NTAGI) has countered these fears and allegations. He said that misinformation was also created during the administering of Polio vaccine in India and abroad that children who are getting the vaccine may face infertility in the future. He assured that all vaccines go through intense scientific researches and none of the vaccines have this sort of side-effect.
(https://pib.gov.in/PressReleseDetailm.aspx?PRID=1730219 )
The National Expert Group on Vaccine Administration for COVID-19 (NEGVAC) has also recommended the COVID-19 vaccination for all lactating women, terming it as safe with no need to stop or pause breastfeeding before or after the vaccination. (https://pib.gov.in/PressReleasePage.aspx?PRID=1719925).
*****
UPU affirms commitment to tackle African postal sector challenges
Speaking in Zimbabwe, the Director General of the Universal Postal Union (UPU) Bishar A. Hussein told an audience from African posts that the UN specialized agency was dedicated to enhancing African postal development.

We continue to collaborate in various activities geared to enhancing postal development in Africa and to strengthen our partnership which has grown from strength to strength. We also come together to celebrate our achievements and to tackle challenges facing the postal sector in Africa,” he said.
The UPU DG spotlighted the intensive work of the UPU’s Regional Project on Operation Readiness for E-commerce (ORE) to assist posts to modernize processes and IT systems. There are 45 African countries participating in the ORE regional project enabling them to contribute to the growth of the e-commerce market.
“The project is geared to ensure that designated postal operators in Africa benefit from the global growth of e-commerce,” Mr. Hussein told the audience.
He pointed to the tremendous progress made under the ORE regional project of the UPU Customs Declaration System (CDS). The system assists posts to exchange messages with their customs authority and other posts using electronic data interchange technology. In 2017, no African country had implemented CDS. Just four years later, as of April 2021, 40 African countries are able to send and receive EDI messages connected to e-commerce items.
The UPU is also channelling support to designated operators in African countries as part of the Regional Project on Digital Transformation and Diversification of Postal Services in Africa. Capacity building workshops and other activities are facilitating the digital transformation of designated postal operators in the region.
In addition to the technical assistance to be provided through the UPU co-operation and development funds, additional financial resources are being mobilised from donors and other partners. The UPU is also exploring opportunities for south-south and triangular cooperation, for the benefit of the region.
The other strategic project being delivered in the region is the Project on Electronic Advanced Data (EAD) funded from the UPU Common Fund.
“EAD’s objective is to build the necessary capacity within designated operators to enable to them to meet the new UPU mandatory regulations on the movement of postal items containing goods,” said Mr. Hussein.
The UPU DG was speaking at the 10th Ordinary Session of the Pan African Postal Union (PAPU) Plenipotentiary Conference.
The Plenipotentiary Conference composed of Ministers in charge of Postal Matters/Communication and Information Technology in Member States, whose ordinary sessions take place every four years to elect the secretary general and the Members of the Administrative Council.
Held in Angel Falls, Zimbabwe, the conference was also attended by President of the Republic of Zimbabwe, Dr. Emmerson Dambudzo Mnangagwa, Minister of ICTs, Postal and Courier Services in Zimbabwe, Dr Jenfan Muswere, the Chairman of PAPU Plenipotentiary Conference, Madam Minette Libom Li Likeng, the UPU Deputy Director General Pascal Clivaz, and the heads of delegations of PAPU member countries.

SB Order 16/2021 - Completion of SOL merger activity for merged CBS post offices

What about the assurances for revision of minimum wage?

Courtesy : The Pioneer , Dated 30.06.2021
What about the assurances for revision of minimum wage?
Wednesday, 30 June 2021 | BRURUHASPATI SAMAL
The Central Government has declared unilateral implementation of the recommendations of 7th Central Pay Commission (CPC) without any modifications through a Cabinet decision on June 29, 2016. This was done, despite repeated correspondences with the Prime Minister, Cabinet Secretary and Secretary DoPT and several rounds of country wide agitational programmes including serving of notice to go for nationwide indefinite strike.
The employees have expressed their serious resentment for wrong interpretation and implementation of Dr Aykroyd Formula approved by the Supreme Court of India to determine the minimum need-based wage which was fixed by the CPC at Rs 18,000 instead of Rs 26,000 as demanded.
In addition, abolition of 52 allowances, merger of 36 allowances with Pay, decrease in percentage of the house rent allowance, no change in annual increment / financial upgradations / casual and maternity leave even after a gap of ten years, 20% decrease in pay in the 2nd year of Child Care leave etc. were some of the negative recommendations of the 7th CPC.
The CPC also ignored the demands of the staff side for revision of minimum wage at 3.7 multiplying factor, 5% annual increment, 5 promotions during the entire service career of an employee etc and above all the understanding in between the staff side and Secretary, DoPT for implementation of the recommendations from 01.01.2014.
Moreover, both the CPC and the Government avoided the demands of as many as 3 lakh Gramin Dak Sewaks and lakhs of casual and contract workers working in the Central Government establishment. However, due to the strong protest by NJCA, the then Union Home Minister Rajnath Singh, as per direction of the Prime Minister held discussions with the NJCA leaders on June 30, 2016 in the presence of Finance Minister Arun Jaitly and Railway Minister Suresh Prabhu.
The National Joint Council of Action (NJCA), is a united forum of more than 120 independent organizations comprising Confederation of Central Government Employees and Workers along with Railway and Defence Federations.
After hours of discussions on the demands with particular reference to revision in minimum wage and Fitment Formula, the group of Cabinet Ministers, without any written minutes or communications just verbally assured that a high-level committee would be appointed to consider the issues raised by the NJCA which prompted the NJCA to go for nationwide Indefinite Strike from July 11, 2016 as notified earlier. Country wide demonstrations were held daily in front of all offices and at all important centres.
On July 6, 2016 when the NJCA meeting was in progress on the preparations of the proposed nationwide strike, the then Home Minister Rajnath Singh again invited the NJCA leaders for discussion in the presence of Finance, Railway and Communication Ministers.
After hours of discussion with 17 staff representatives of the NJCA, the group of Ministers reiterated the earlier assurances of the Government basing on which the proposed indefinite strike commencing July 11, 2016 was deferred. However, while answering to the Unstarred Question No. 1170 put in this regard in Rajya Sabha, the then Union Finance Minister (State) P Radhakrishnan replied on March 6, 2018 in contradiction to the written assurances of a group of Cabinet Ministers.
He said, “The minimum pay of Rs 18,000 pm and fitment factor of 2.57 are based on the specific recommendations of the 7th Central Pay Commission in the light of the relevant factors taken into account by it. Therefore, no change therein is at present under consideration”. In the meantime, more than 5 years have passed. No action has yet been taken either to constitute the proposed committee nor to have a negotiation with the staff side representatives.
The Confederation of Central Government Employees and Workers has already gone twice for one-day nationwide strike on January 8, 2020 and November 26, 2020 reminding the Central Government of the the discussions and assurances of June 30, 2016 and July 6, 2016 along with demand for 5 years wage revision like banks, insurance and PSUs. But adding salt to the injury, the Central Government has frozen the Dearness Allowance of the employees for 18 months from January 1, 2020 to June 30, 2021 on the plea of Covid-19 pandemic management which is a strong kick of gross injustice on the bread and butter of the employees who are now working in tandem with the Government, administration and the people of the country to fight against Corona. If the written assurances are not kept and DA is not restored immediately, the Confederation and NJCA may once again take a strong decision to go for nationwide agitation culminating to indefinite strike.
(The writer is all India organising general secretary, National Federation of Postal Employees-P-III)
Tuesday, 29 June 2021




MHA Order Dt. 29.6.2021 for containment of Covid 19





Link : https://www.mha.gov.in/sites/default/files/MHAOrder_2962021.pdf




ସରକାରୀ କର୍ମଚାରୀମାନେ ପ୍ରତ୍ୟକ୍ଷ ବା ପରୋକ୍ଷରେ ରାଜନୀତି ସହିତ ସଂଶ୍ଳିଷ୍ଟ ହେବା ଉଚିତ ନୁହେଁ

Courtesy : The Samaja, dated 29.06.2021
Monday, 28 June 2021
Delta and Delta Plus Variants: Frequently Asked Questions
Ministry of Health and Family Welfare
Delta and Delta Plus Variants: Frequently Asked Questions
Posted On: 28 JUN 2021 2:52PM by PIB Mumbai
New Delhi / Mumbai, 28th June, 2021
Vaccines and COVID Appropriate Behaviour can help us fight the pandemic.
Secretary, Department of Biotechnology; Director General, Indian Council of Medical Research; and Director, National Centre for Disease Control have answered many questions about the Delta and Delta Plus variants of the SARS-Cov-2 virus. PIB has curated the answers, given at a COVID Media Briefing held by the Health Ministry on June 25, 2021.
Q. Why does a virus mutate?
Virus by its very nature mutates. It is part of its evolution. The SARS-Cov-2 virus is a single-stranded RNA virus. So, changes in the genetic sequence of the RNA are mutations. The moment a virus enters its host cell or a susceptible body, it starts replicating. When the spread of infection increases, the rate of replication also increases. A virus that has got a mutation in it is known as a variant.
Q. What is the impact of mutations?
The normal process of mutations begins to impact us when it leads to changes in transmission levels or on treatment. Mutations can have positive, negative or neutral effects on human health.
Negative impacts include clustering of infections, increased transmissibility, ability to escape immunity and infect someone who has prior immunity, neutralization escape from monoclonal antibodies, improved binding to lung cells and increased severity of infection.
Positive impacts can be that the virus becomes non-viable.
Q. Why are frequent mutations seen in SARS-CoV-2 virus? When will the mutations stop?
SARS-CoV-2 can mutate due to the following reasons:
- Random error during replication of virus
- Immune pressure faced by viruses after treatments such as convalescent plasma, vaccination or monoclonal antibodies (antibodies produced by a single clone of cells with identical antibody molecules)
- Uninterrupted transmission due to lack of COVID-appropriate behaviour. Here the virus finds excellent host to grow and becomes more fit and more transmissible.
The virus will continue to mutate as long as the pandemic remains. This makes it all the more crucial to follow COVID appropriate behavior.
Q. What are Variants of Interest (VoI) and Variants of Concern (VoC)?
When the mutations happen – if there is any previous association with any other similar variant which is felt to have an impact on public health – then it becomes a Variant under Investigation.
Once genetic markers are identified which can have association with receptor binding domain or which have an implication on antibodies or neutralizing assays, we start calling them as Variants of Interest.
The moment we get evidence for increased transmission through field-site and clinical correlations, it becomes a Variant of Concern. Variants of concern are those that have one or more of the following characteristics:
- Increased transmissibility
- Change in virulence/ disease presentation
- Evading the diagnostics, drugs and vaccines
The 1st Variant of Concern was announced by the UK where it was found. Currently there are four variants of concern identified by the scientists - Alpha, Beta, Gamma and Delta.
Q. What are Delta and Delta Plus variants?
These are the names given to variants of SARS-CoV-2 virus, based on the mutations found in them. WHO has recommended using letters of the Greek Alphabet, i.e., Alpha (B.1.1.7), Beta (B.1.351), Gamma (P.1), Delta (B.1.617), etc., to denote variants, for easier public understanding.
Delta variant, also known as SARS-CoV-2 B.1.617, has about 15-17 mutations. It was first reported in October 2020. More than 60% of cases in Maharashtra in February 2021 pertained to delta variants.
It is the Indian scientists who identified the Delta Variant and submitted it to the global database. Delta variant is classified as a Variant of Concern and has now spread to 80 countries, as per WHO.
Delta variant (B.1.617) has three subtypes B1.617.1, B.1.617.2 and B.1.617.3, among which B.1.617.1 and B.1.617.3 have been classified as Variant of Interest, while B.1.617.2 (Delta Plus) has been classified as a Variant of Concern.
The Delta Plus variant has an additional mutation in comparison to Delta variant; this mutation has been named as the K417N mutation. ‘Plus’ means an additional mutation has happened to the Delta variant. It does not mean that the Delta Plus variant is more severe or highly transmissible than the Delta variant.
Q. Why has the Delta Plus Variant (B.1.617.2) been classified as a Variant of Concern?
The Delta Plus variant has been classified as Variant of Concern because of the following characteristics:
- Increased transmissibility
- Stronger binding to receptors of lung cells
- Potential reduction in monoclonal antibody response
- Potential post vaccination immune escape
Q. How often are these mutations studied in India?
Indian SARS-CoV-2 Genomics Consortium (INSACOG) coordinated by the Department of Biotechnology (DBT) along with Union Health Ministry, ICMR, and CSIR monitor the genomic variations in the SARS-CoV-2 on a regular basis through a pan India multi-laboratory network. It was set up with 10 National Labs in December 2020 and has been expanded to 28 labs and 300 sentinel sites from where genomic samples are collected. The INSACOG hospital network looks at samples and informs INSACOG about the severity, clinical correlation, breakthrough infections and re-infections.
More than 65,000 samples have been taken from states and processed, while nearly 50,000 samples have been analysed of which 50% have been reported to be Variants of Concern.
Q. On what basis are the samples subjected to Genome Sequencing?
Sample selection is done under three broad categories:
1) International passengers (during the beginning of the Pandemic)
2) Community surveillance (where RT-PCR samples report CT Value less than 25)
3) Sentinel surveillance - Samples are obtained from labs (to check transmission) and hospitals (to check severity)
When there is any public health impact noticed because of genetic mutation, then the same is monitored.
Q. What is the trend of Variants of Concern circulating in India?
As per the latest data, 90% of samples tested have been found to have Delta Variants (B.1.617). However, B.1.1.7 strain which was the most prevalent variant in India in the initial days of the pandemic has decreased.
Q. Why public health action is not taken immediately after noticing mutations in virus?
It is not possible to say whether the mutations noticed will increase transmission. Also, until there is scientific evidence that proves a correlation between rising number of cases and variant proportion, we cannot confirm there is a surge in the particular variant. Once mutations are found, analysis is made week on week to find if there is any such correlation between the surge of cases and variant proportion. Public health action can be taken only after scientific proofs for such correlation are available.
Once such correlation is established, this will help greatly to prepare in advance when such variant is seen in another area/region.
Q. Do COVISHIELD and COVAXIN work against the variants of SARS-CoV-2?
Yes, COVISHIELD and COVAXIN are both effective against the Alpha, Beta, Gamma and Delta variants. Lab tests to check vaccine effectiveness on Delta Plus Variant are ongoing.
Delta Plus Variants: The virus has been isolated and is being cultured now at ICMR’s National Institute of Virology, Pune. Laboratory tests to check vaccine effectiveness are ongoing and the results will be available in 7 to 10 days. This will be the first result in the world.
Q. What are the public health interventions being carried out to tackle these variants?
The public health interventions needed are the same, irrespective of the variants. The following measures are being taken:
- Cluster containment
- Isolation & Treatment of cases
- Quarantining of contacts
- Ramping up vaccination
Q. Do public health strategies change as the virus mutates and more variants arise?
No, public health prevention strategies do not change with variants.
Q. Why is continuous monitoring of mutations important?
Continuous monitoring of mutations is important to track potential vaccine escape, increased transmissibility and disease severity.
Q. What does a common man do to protect him/her from these Variants of Concern?
One must follow COVID Appropriate Behaviour, which includes wearing a mask properly, washing hands frequently and maintaining social distancing.
The second wave is not over yet. It is possible to prevent a big third wave provided individuals and society practise protective behaviour.
Further, Test Positivity Rate must be closely monitored by each district. If the test positivity goes above 5%, strict restrictions must be imposed.
***
Subscribe to:
Comments (Atom)